
Why it’s hard to tell schizophrenia and HPPD apart and what this article will do for you
Imagine seeing things that aren’t there or feeling like the world around you isn’t quite real.

These are scary feelings, and they can make you wonder what’s happening. Many people worry that these might be signs of serious conditions like schizophrenia. But sometimes, these feelings can be caused by something else entirely, such as Hallucinogen Persisting Perception Disorder, often called HPPD.
It’s actually quite common for people to get confused between these two. The main reason is that both conditions can cause you to experience changes in your senses. You might see patterns, colors, or movements that others don’t, or feel a strange detachment from your body. These kinds of symptoms can make it very hard to know if you’re experiencing early symptoms of schizophrenia or if it’s something different like HPPD. The way mental health conditions are understood and diagnosed can also be complex, as noted in discussions about the Diagnostic and Statistical Manual of Mental Disorders, or DSM-5, which provides guidelines for doctors Diagnostic Issues and Controversies in DSM-5.
This article is here to help clear up that confusion. We will go through the key symptoms of schizophrenia and explain what makes them different from hallucinogen persisting perception disorder. You’ll get a clear, step-by-step guide to understanding the differences and learn about other conditions, like schizoaffective disorder symptoms, that sometimes look similar. We’ll also talk about the specific signs or "red flags" that mean you should really see a doctor for a psychiatric evaluation form. Knowing these things can help you understand what’s going on and decide the best next steps for your health.
If you’re trying to figure out if your symptoms point to one or the other, this guide will help you understand Schizophrenia or HPPD: Which One Is Causing Your Symptoms?.
Feeling emotionally drained? The pressure may not be only personal. Feeling Emotionally Drained?
What are schizophrenia spectrum disorders? (A plain-language primer)
When we talk about schizophrenia spectrum disorders, we’re actually talking about a group of serious brain illnesses. These conditions change how a person thinks, feels, and acts. It’s not just one thing; it’s a range of issues that affect how someone understands the world around them. Doctors use special guidelines like the DSM-5 to help figure out what kind of problem someone is facing fifth edition – dsm-5.
The symptoms of schizophrenia can be split into a few main types:
- Positive Symptoms: These are things that are "added" to a person’s experience that shouldn’t be there.
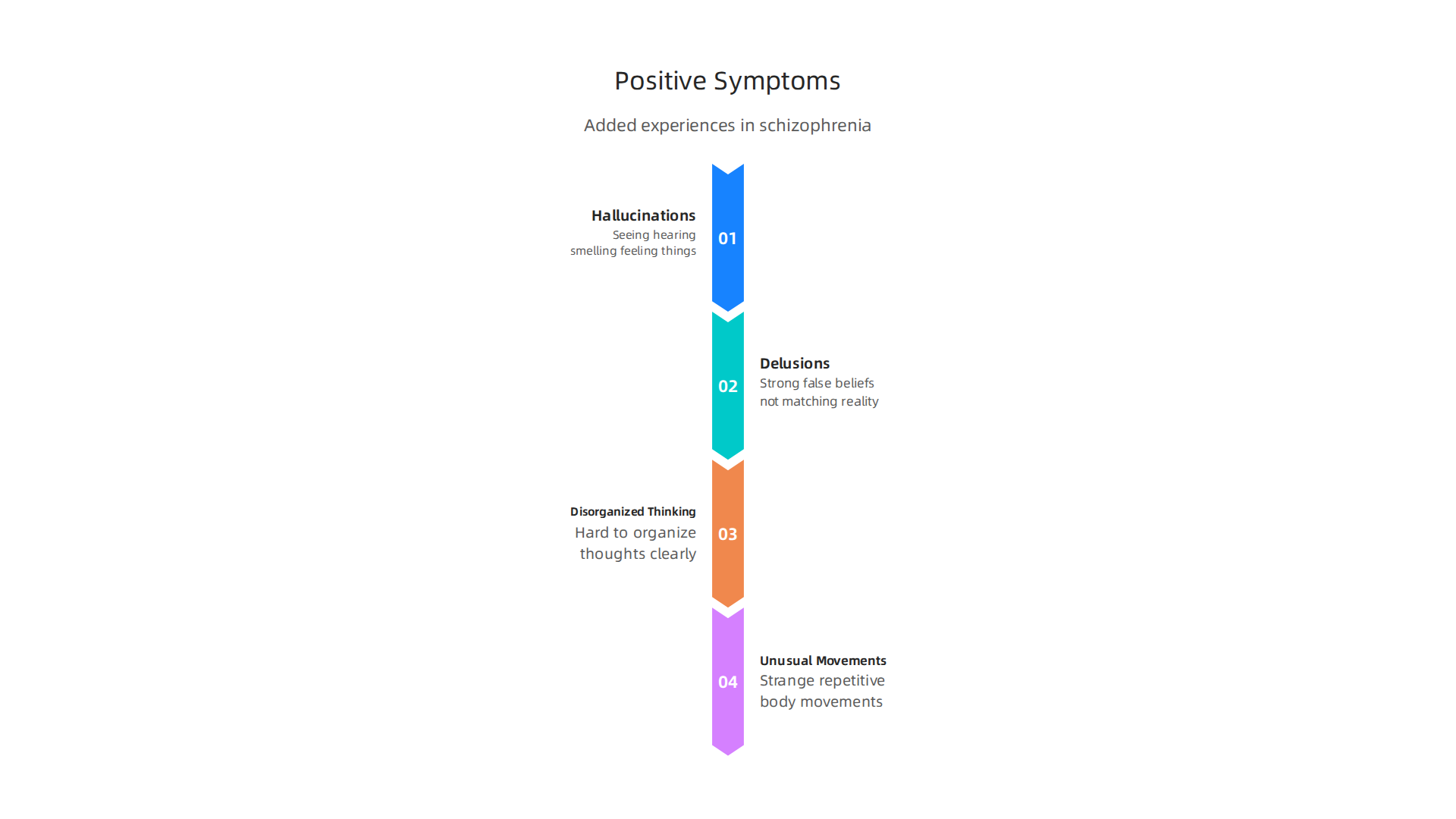
* **Hallucinations:** This means seeing, hearing, smelling, tasting, or feeling things that aren't real. A common one is hearing voices.
* **Delusions:** These are very strong, false beliefs that don't match reality. For example, a person might believe they are famous or that someone is trying to harm them.
* **Disorganized Thinking:** It can be hard for someone to put their thoughts together clearly. Their speech might jump from one idea to another, making it tough to understand them.
* **Unusual Movements:** This might look like strange body movements, repeating certain actions, or even staying very still for a long time.
-
Negative Symptoms: These are things that are "taken away" or reduced from a person’s normal self.
- Lack of Emotion: A person might show very little emotion, like having a flat voice or not changing their facial expressions much.
- Low Motivation: It can be very hard to start or keep up with daily activities.
- Loss of Pleasure: Things that used to be fun might not bring joy anymore.
- Social Withdrawal: People might pull away from friends and family.
-
Cognitive Changes: These are problems with how a person thinks. They might have trouble with memory, find it hard to pay attention, or struggle to plan things or make decisions.
Together, these symptoms of schizophrenia can make it very hard for someone to live their daily life.

They might struggle at school or work, or find it difficult to keep friendships. The problems often start slowly, making them hard to notice at first. Usually, schizophrenia spectrum disorders appear in someone’s late teens or early 30s. While rare, sometimes these conditions can affect children and teenagers, which brings its own challenges for doctors to diagnose Trends and diagnostic challenges in pediatric schizophrenia ….
Sometimes, people also hear about schizoaffective disorder symptoms. This is another type of disorder in the schizophrenia spectrum. It means a person has symptoms of schizophrenia, but also has strong mood problems, like very low moods (depression) or very high moods (mania). Recognizing these early signs, which often include changes in thinking and perception, is crucial for getting help, especially when psychosis symptoms are present. You can learn more about recognizing these important warning signs and finding support in our guide to Psychosis Symptoms: Recognizing Early Warning Signs and Getting Help.
While the symptoms of schizophrenia involve changes in thinking and perception that are not tied to substance use, there’s another condition that causes similar types of visual disturbances. It’s called Hallucinogen Persisting Perception Disorder or HPPD.
HPPD is a rare problem where a person keeps seeing or feeling things that aren’t real, long after they’ve used hallucinogenic drugs. Think of drugs like LSD or magic mushrooms. Even if someone hasn’t used these drugs for months or years, they might still have "visual flashbacks" or other sensory issues Historical Development and Current Use of the Term “Flashback” in….
It’s not the same as being high on the drug or going through withdrawal. Instead, these strange perceptions stick around for a long time HALLUCINOGENS AND DISSOCIATIVE DRUGS.
What kind of things do people with HPPD see?
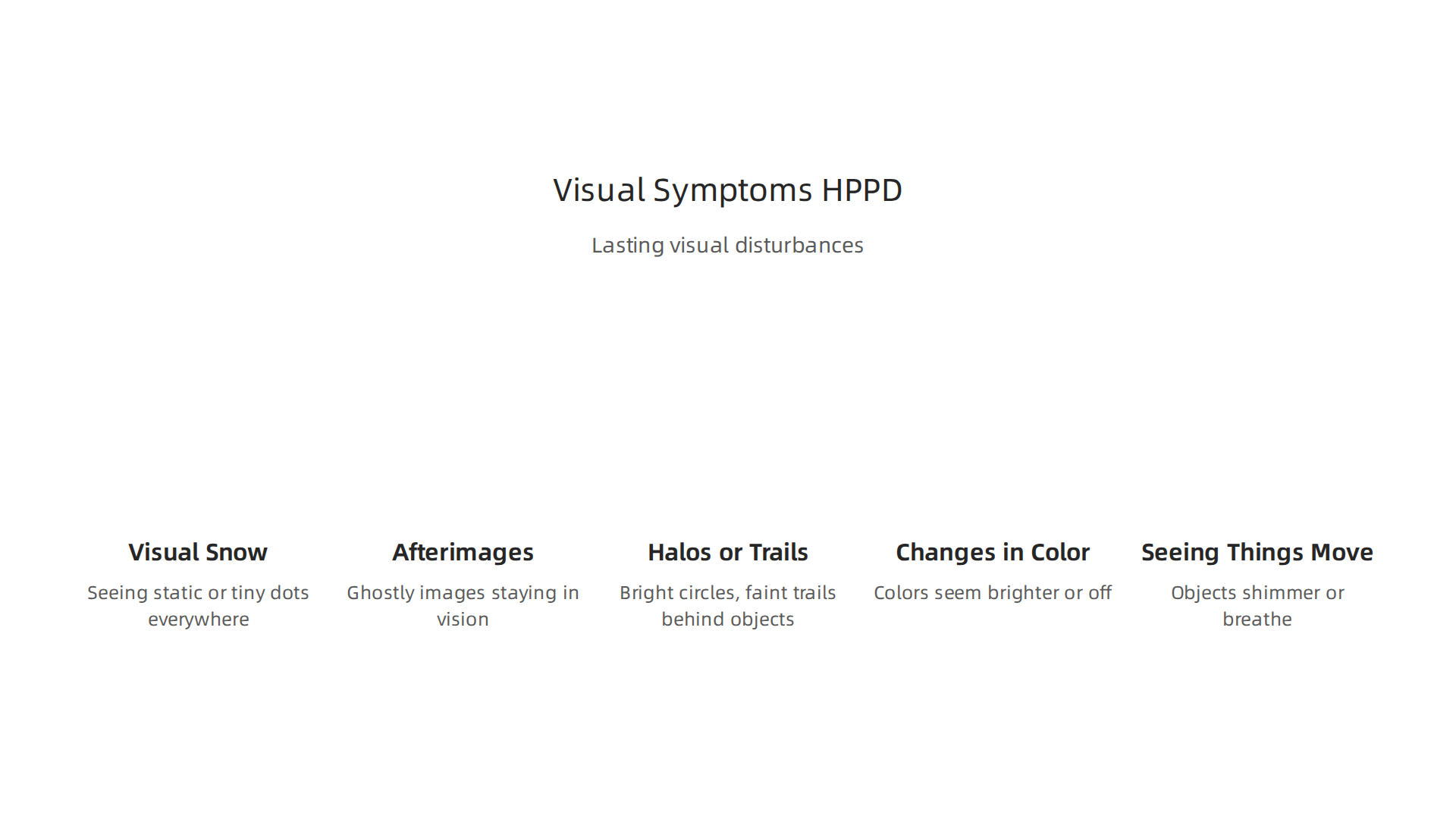
- Visual Snow: This is like seeing static or tiny dots, similar to an old TV screen, everywhere they look.
- Afterimages: When they look away from something bright, a ghostly image of it might stay in their vision for a while.
- Halos or Trails: Lights might have bright circles around them, or moving objects might leave a faint trail behind them.
- Changes in Color: Colors might seem brighter, duller, or just "off."
- Seeing things move: Still objects might appear to shimmer or breathe.
These sights can be annoying or even scary. They’re not delusions, where a person believes something false; the person often knows these things aren’t real, but they can’t make them stop. The symptoms can come and go, or they can be constant.
It’s important to know that HPPD is different from other mental health problems like schizoaffective disorder symptoms or even psychosis related to drug use that goes away once the drug is out of the system. While both HPPD and symptoms of schizophrenia can involve changes in perception, their causes and treatments are usually very different Clinical characteristics of individuals with schizophrenia and hallucinogen persisting perception disorder. If someone is experiencing these kinds of lasting visual changes after drug use, they should talk to a doctor or mental health professional. It’s really important to get a clear diagnosis, perhaps through a detailed psychiatric evaluation form, to figure out what’s really going on. You can learn more about how these two conditions compare by reading our guide on Schizophrenia or HPPD: Which One Is Causing Your Symptoms.
Sometimes, finding the right mental health care can feel like a maze. If you’re wondering about how to pay for treatment, check out How to Navigate Mental Health Insurance Billing and Afford Therapy in 2026.
Overlapping symptoms: How HPPD and schizophrenia can look similar
It can be really tricky to tell the difference between hallucinogen persisting perception disorder (HPPD) and actual symptoms of schizophrenia because some of their signs can seem very much alike. Both conditions can make a person see or hear things that aren’t there, or experience other strange perceptions. This is why getting a clear diagnosis from a doctor is so important.
Here are some ways HPPD and the symptoms of schizophrenia might seem similar:
- Seeing Things That Aren’t Real: People with HPPD often see "visual snow," halos, or trails, as we talked about before. In schizophrenia, people can also have visual hallucinations. Both conditions make the world look different than it really is.
- Changed Perceptions: Beyond just seeing things, both conditions can cause things to look distorted. Colors might seem off, or still objects might appear to move or breathe. This makes it hard to trust what their eyes are telling them.
- Feeling Worried or Scared: When you’re constantly seeing things that others don’t, it can be very upsetting. This often leads to a lot of worry and fear, which can sometimes make the strange perceptions feel even more real or scary. This anxiety can be mistaken for other mental health issues.
- "Psychotic-like" Moments: Sometimes, the severe visual issues in HPPD can feel like a brief, confusing episode that resembles psychosis. Psychosis is when someone loses touch with reality. While HPPD usually means a person knows what they are seeing isn’t real, the constant strange sights can still be very confusing and make them question their sanity, which can look a lot like true schizoaffective disorder symptoms in some ways.
Why It’s Hard to Tell Them Apart
Because of these overlaps, it’s really tough for doctors to figure out what’s going on without a full picture. Here’s why:
- Drug Use History: Doctors need to know if the person has ever used hallucinogenic drugs. If they have, HPPD is a possible answer. But if they haven’t, or if their problems started long before drug use, it points more towards conditions like schizophrenia.
- When Symptoms Started: Did the strange sights begin right after drug use and then stick around? Or did they appear gradually without any clear cause? The timing helps doctors guess if it’s HPPD or something else.
- How Symptoms Change Over Time: HPPD symptoms tend to be mostly visual and don’t usually get worse over time in the same way that schizophrenia can. Schizophrenia often involves more than just visual problems, like changed thinking and hearing voices, and these issues can get worse without help.
Getting an accurate diagnosis is the first and most important step to getting the right kind of help. If you or someone you know is having these kinds of experiences, a doctor or mental health professional can help sort it out, perhaps using a detailed psychiatric evaluation form to gather all the important information.
Feeling Emotionally Drained? The pressure may not be only personal. Learn more about how outside factors can affect your well-being at Dean Grey’s blog.
It can be tough for doctors to tell the difference between these conditions, but they look for special clues.
They carefully check a person’s history and the specific kinds of problems they are having. This helps them know if it’s the symptoms of schizophrenia or hallucinogen persisting perception disorder (HPPD).
When Things Started and Drug Use
One of the biggest clues is when the symptoms began.
- HPPD: This problem usually starts right after someone has used hallucinogenic drugs. The strange sights and perceptions show up soon after the drug use and just keep happening. It’s often very clear that the drug use triggered the symptoms. Doctors need to know if a person has used these types of drugs to consider HPPD.
- Schizophrenia: The symptoms of schizophrenia often start slowly, over time, without any clear trigger like drug use. A person might slowly feel worse, have trouble thinking, or find it hard to do their usual daily tasks. This can happen little by little, making it harder to pinpoint an exact start date.
Knowing if and when someone used hallucinogens is a key piece of the puzzle. Without this drug history, HPPD is much less likely.
Different Kinds of Symptoms
While both can cause strange perceptions, the types of symptoms are often different.
- HPPD: People with HPPD mostly have visual problems. They might see things that aren’t there, like patterns or bright spots, or things might look wavy or move. But here’s an important point: they usually know that what they are seeing isn’t real. Their thinking and beliefs don’t usually get mixed up. These problems stay mostly about what they see.
- Schizophrenia: This condition involves much more than just seeing things. People with schizophrenia can have strange beliefs that are not true, even when shown facts (these are called fixed delusions). Their thoughts might get jumbled, making it hard for them to speak clearly or follow conversations. They might also hear voices or other sounds that aren’t there. Plus, some people with schizophrenia might also have "negative symptoms," which means they show less emotion, have little motivation, or don’t enjoy activities they once loved. These kinds of symptoms are generally not part of HPPD. A doctor might look for these differences to make a careful diagnosis, as outlined in studies comparing the conditions like those found in "Should People With a History of Psychosis Be Included in … – Érudit" from 2026.
By looking closely at these differences, especially the timing of symptoms and the types of problems a person is having, doctors can figure out the best way to help.
When things are already tough, knowing when to get help can feel like another big worry. But there are clear signs that mean it’s time to talk to a doctor or mental health expert. It’s really important to seek help right away if you notice these things getting worse for yourself or someone you care about.
When to Seek Help
Here are some red flags that mean it’s time for a professional to step in:
- Big Trouble in Daily Life: If you find it very hard to do everyday things like go to work or school, take care of yourself, or keep up with friends and family. This is called a functional decline. The symptoms of schizophrenia or even schizoaffective disorder symptoms can make daily life very difficult.
- Thoughts of Harming Yourself or Others: If you or someone you know is thinking about hurting themselves or someone else, this is a very serious emergency. Please call 911 right away or reach out to a crisis hotline. You can find a helpful Non-Emergency Phone Number List for Depression and Mental Health Crises for mental health support.
- Strange Perceptions That Get Worse: If you keep seeing or hearing things that aren’t real, or have very strong beliefs that no one can change, and you’re not sure what’s real anymore. This is especially true if these feelings are getting stronger or happening more often. This can be very unsettling.
What to Expect at a Professional Evaluation
When you see a doctor or a mental health expert for these concerns, they will do a careful check-up.

This often includes:
- Asking About Your History: They will ask many questions about your health, your family’s health, and how things have been going in your life. They want to understand your full story.
- Talking About Substance Use: The doctor will ask about any drugs or alcohol you might have used. They need to know the timeline of this use, especially if they are looking into something like hallucinogen persisting perception disorder, which can be related to past drug use.
- A Mental Status Exam: This is not a test with right or wrong answers. It’s a way for the doctor to observe how you think, feel, and behave during your talk. They’ll pay attention to your mood, how clearly you speak, and how you see the world.
- Using Special Forms: Doctors often use specific questions or a psychiatric evaluation form to make sure they gather all the important details needed for an accurate diagnosis.
- Possible Referrals: After the evaluation, the doctor might suggest you see other specialists, like a psychiatrist or a therapist, for more help. Learning about different AMP Mental Health Providers Guide to Psychiatrists, Therapists, and Counselors can help you know what to expect.
Getting a clear evaluation is the first step toward getting the right help and feeling better.
After a doctor or mental health expert talks with you and asks about your life, they often use special tools to help them understand what’s going on. These tools are like careful checklists and interviews designed to spot certain patterns. They are very helpful, especially when trying to understand conditions like the symptoms of schizophrenia or other related issues.
Screening Tools and Interviews
Doctors use what are called "screening tools" and "structured interviews." These are not just casual chats. They are sets of specific questions that help find early signs of problems, like early psychosis. For example, some tools help clinicians look for patterns that match schizoaffective disorder symptoms or other difficulties. There are even self-screening questionnaires that people can use themselves, which can be a first step to noticing if something is wrong. These methods help make sure all important details are covered, much like a general psychiatric evaluation form ensures a thorough review.
To make a correct diagnosis, doctors use guides like the "Diagnostic and Statistical Manual of Mental Disorders" (DSM-5-TR), which is like a big book of rules and descriptions for mental health conditions. It helps them compare your symptoms to known conditions, ensuring they give you the best possible diagnosis. The DSM-5-TR is updated often, with the latest guidelines helping doctors in 2026 make accurate diagnoses. You can learn more about recognizing possible signs by understanding psychosis symptoms and seeking timely help.
These tools are also important for looking into things that might seem like psychosis but are actually caused by other factors. For example, some people might experience lasting visual changes after using certain drugs. This is known as hallucinogen persisting perception disorder, and it requires careful screening to tell it apart from other conditions.
Imaging and Lab Tests
Sometimes, doctors might suggest imaging tests, like an MRI of your brain, or blood tests. It’s important to know that these tests usually do not directly diagnose conditions like the symptoms of schizophrenia or schizoaffective disorder. Mental health conditions are mostly diagnosed by talking to you and observing your behavior and thoughts.
However, these tests can be very useful for a different reason: they help rule out other medical problems that might be causing your symptoms. For example, a brain tumor, an infection, or even a vitamin deficiency can sometimes cause symptoms that look like mental illness. Imaging and blood tests can check for these physical causes. If the tests show nothing wrong physically, then the doctor can be more sure that your symptoms are related to a mental health condition. This helps them focus on the right kind of treatment for you.
After a doctor has a clear picture of your condition, the next step is to talk about how to help you feel better. Treatment plans are often different depending on the specific mental health challenge.
Treatment approaches and immediate support options
For conditions like the symptoms of schizophrenia or schizoaffective disorder symptoms, treatment usually involves a two-part approach. The first part often includes medications called antipsychotics. These medicines can help reduce strong symptoms like hallucinations and delusions. Experts agree that antipsychotic medications are a main way to treat schizophrenia, helping to lower how bad symptoms are and stop them from coming back often Psychosocial Treatments for Schizophrenia.
The second, equally important part is called psychosocial treatment. This includes different types of therapy, like talking to a counselor, joining support groups, or learning life skills. These helps people manage their thoughts, feelings, and daily life. It’s often found that treating psychosis and similar disorders needs both therapy and medicine together Psychosocial Interventions for Psychosis and Psychotic Disorders in Youth.
However, conditions like hallucinogen persisting perception disorder (HPPD) are treated differently. Since HPPD is usually about lasting changes in how you see things after drug use, its treatment focuses more on managing those symptoms and providing psychological support. This might include therapies that help you cope with visual changes and anxiety, rather than relying on antipsychotic medicines as the first choice.
Getting immediate help
While waiting for a full diagnosis and treatment plan, there are important steps you and your caregivers can take. If someone is going through a mental health crisis, it’s key to make sure they are safe. This means keeping dangerous items away and staying calm. Talking openly about what’s happening can help, but don’t force it.
It’s also important to reach out for help. You can call a doctor or mental health professional right away. For moments of deep distress, knowing who to call can make a big difference. Check out a Non-Emergency Phone Number List for Depression and Mental Health Crises for helpful contacts. Learning about Mental Health First Aid can also teach you simple actions to take during emotional crises. Remember, you don’t have to face these challenges alone.
Summary
This article explains why Hallucinogen Persisting Perception Disorder (HPPD) and schizophrenia can look similar and how clinicians tell them apart. It reviews the core positive, negative, and cognitive symptoms of schizophrenia and contrasts them with the mostly visual disturbances seen in HPPD, such as visual snow, afterimages, halos, and trails. The guide emphasizes why timing and a history of hallucinogen use are often decisive, outlines what to expect during a psychiatric evaluation, and describes screening tools, imaging, and lab tests used to rule out other causes. You’ll also learn which warning signs require immediate help, how treatment differs (antipsychotics plus psychosocial care for schizophrenia versus symptom management and therapy for HPPD), and practical steps for getting accurate diagnosis and care. By the end, readers should be able to describe key differences, know when to seek help, and find relevant next steps and resources.
